

Too many aggressive prostate cancers are missed
Prostate cancer is a major cause of cancer-related deaths. PSA screening misses aggressive cancers in men with low levels, while higher PSA levels often are unrelated to cancer.
Stockholm3 Benefits:
• Designed for early detection and screening
• 60% fewer prostate cancer deaths at six years follow-up
• Identifies aggressive cancer missed by PSA
• 90% sensitivity for aggressive disease
• Designed for early detection and screening • 60% fewer prostate cancer deaths at six years follow-up • Identifies aggressive cancer missed by PSA • 90% sensitivity for aggressive disease
The limitations of PSA screening
PSA screening has saved lives by detecting aggressive cancers early, but also has important limitations.
A major problem is that it misses aggressive cancers in men with low PSA levels (below 3-4 ng/mL).[1]
Up to 50% of aggressive prostate cancers occur at low PSA levels. [2,3,4]
PSA can also rise for reasons unrelated to cancer, and has limited ability to distinguish between slow-growing, harmless cancers and aggressive cancers that require treatment. This leads to false alarms causing unnecessary magnetic resonance imaging (MRI) scans, biopsies, anxiety, and healthcare costs. [5]


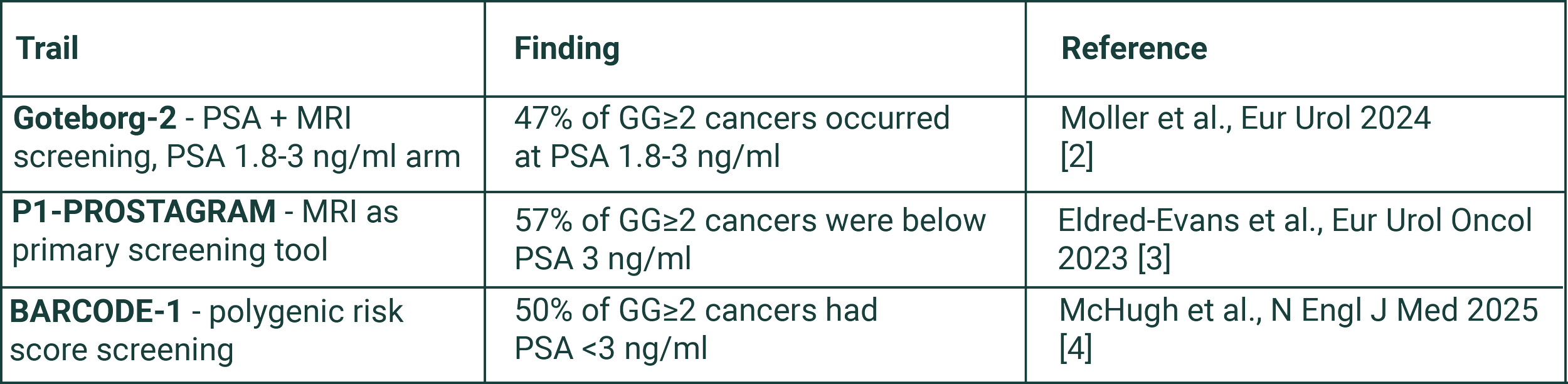
Up to 50% of aggressive cancers occur at low PSA levels (<3 ng/ml)
Supporting evidence - aggressive (Grade Group ≥2) cancers detected at low PSA
A next generation screening test
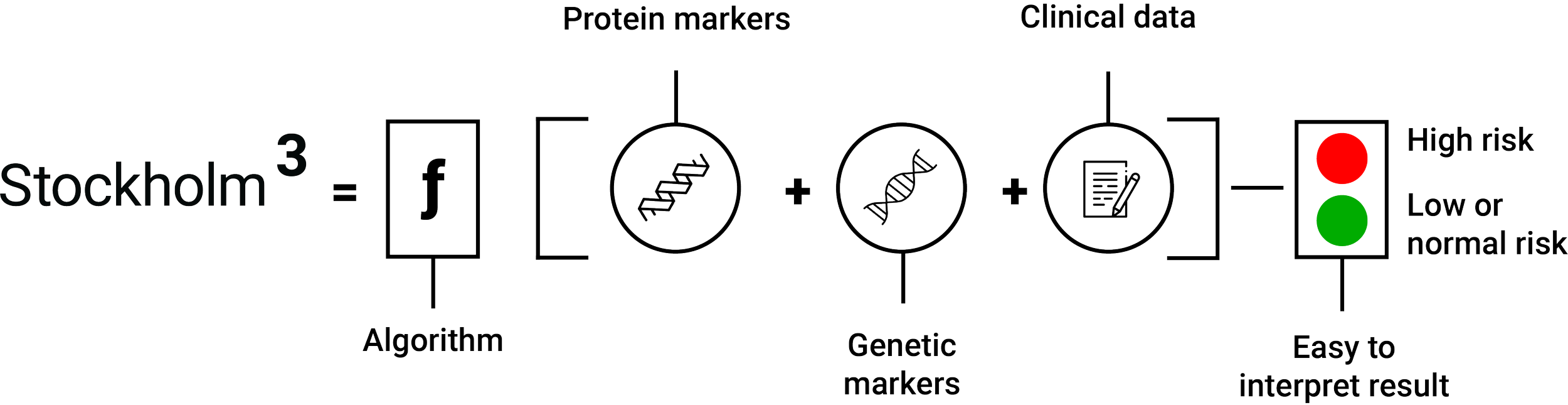
Stockholm3 is a blood-based test that combines protein biomarkers, genetic risk, and clinical factors to estimate a man’s risk of having aggressive prostate cancer. [6,7]
Stockholm3 can replace PSA as a more precise screening tool by finding aggressive cancers (defined as ISUP Grade Group ≥ 2) earlier while reducing the over-detection that has historically limited prostate cancer screening.
By clarifying risk earlier in the screening process, Stockholm3 enables more appropriate follow-up. Men at higher risk can be identified earlier, while men at low risk can avoid unnecessary diagnostic pathways.
Finding more aggressive cancers while curable
Stockholm3 Benefits:
Improved screening and early detection of aggressive prostate cancer [6,8,9]
Identifies aggressive disease missed by standard PSA thresholds [9,10,11]
Fewer unnecessary procedures in low-risk men [8,12,13,14]
Stage migration towards more curable disease [10,15,16]
Built for large-scale clinical implementation
Stockholm3 uses a standard blood draw and can easily be integrated in existing clinical workflows. The outcome is an individualized and actionable prostate cancer risk score. An elevated Stockholm3 Risk Score indicates an increased risk of aggressive prostate cancer, supporting further diagnostic workup such as MRI or prostate biopsy in accordance with current medical practice.

Backed by substantial clinical evidence
Stockholm3 has been evaluated in high quality studies including 90,000 men and in clinical care. [6,8,10,12,13,14,15,17,18]
Findings from prospective screening studies, large-scale real-world implementation and long-term follow-ups point in the same direction: improved early detection of aggressive prostate cancer, better risk discrimination, and fewer prostate cancer related deaths. [8,9,10,11,15,16]
90% sensitivity in prostate cancer screening
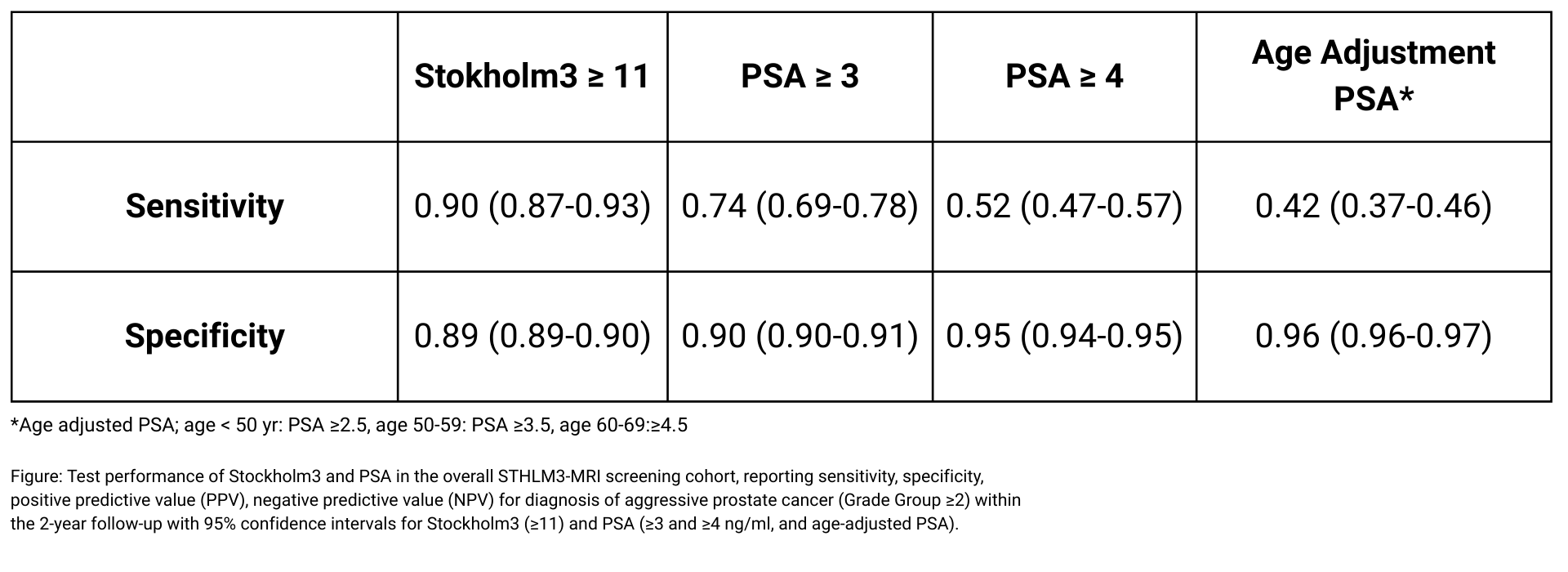
In a large prospective screening study (N=12,670), Stockholm3 demonstrated 90% sensitivity for detecting aggressive prostate cancer. This performance significantly outperforms PSA thresholds at comparable specificity. [8,9]
Follow-up from screening studies suggests evidence of nearly 60% reduced prostate cancer mortality (instrumental-variable analysis RR: 0.41; 95% CI: 0.18-0.91) when Stockholm3 is used compared with PSA-based screening.[16]
This improvement in survival appears to be driven by earlier detection of biologically aggressive cancers that are frequently missed by conventional PSA use.
Long term follow-up suggests reduced prostate cancer deaths
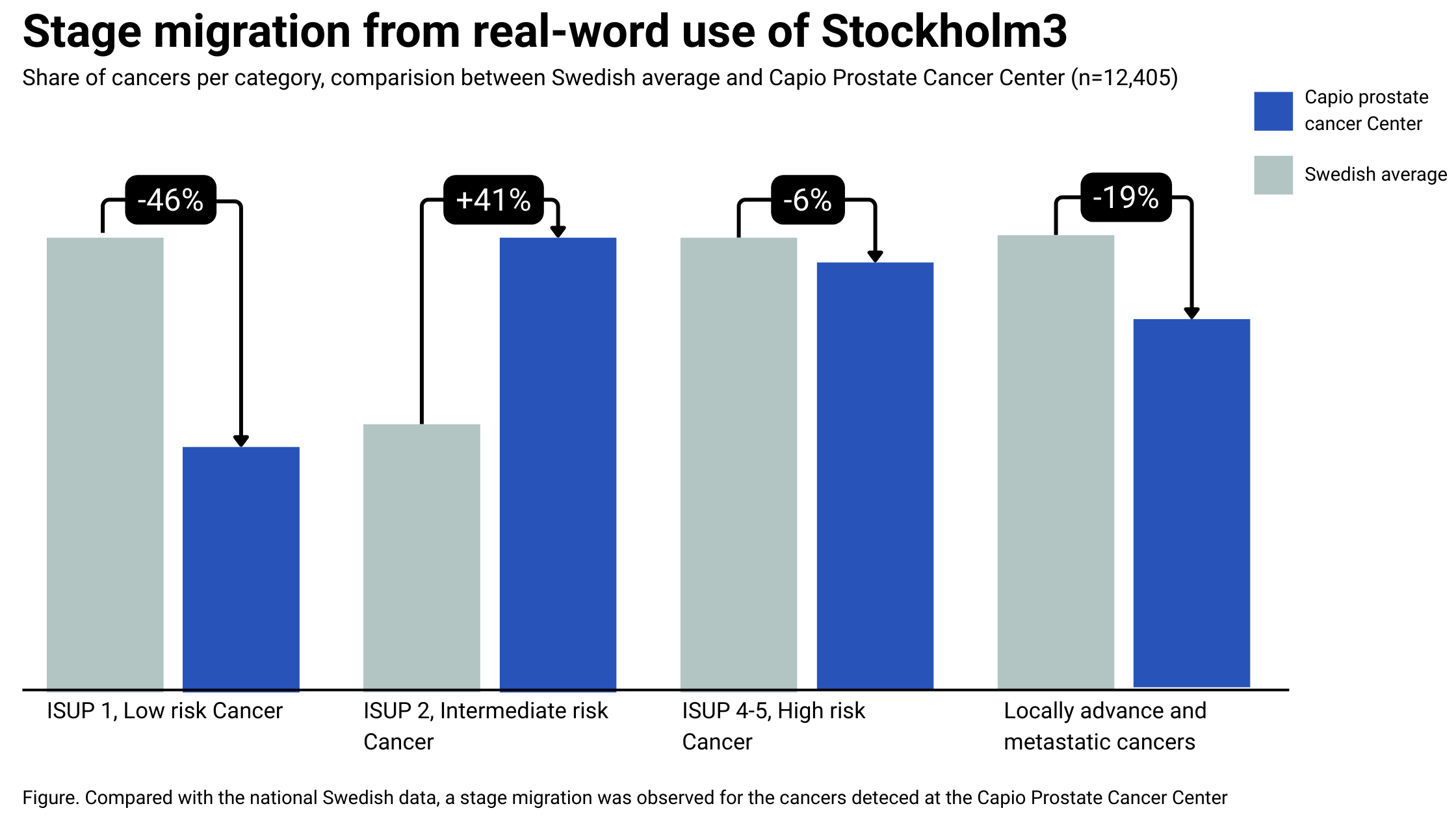
Real-world performance at scale
Real-world use of Stockholm3 has led to stage migration toward more curable disease and less indolent and advanced disease.

Real-World use Norwegian health system (N=4,784)
Replacing PSA with Stockholm3 led to an 89% increase in the detection of aggressive prostate cancer and a 26% reduction in the detection of indolent disease. [15]
Real-world use Swedish Health system (N=12,405)
Replacing PSA with Stockholm3 led to stage migration toward more curable disease and less indolent and advanced disease. [10]
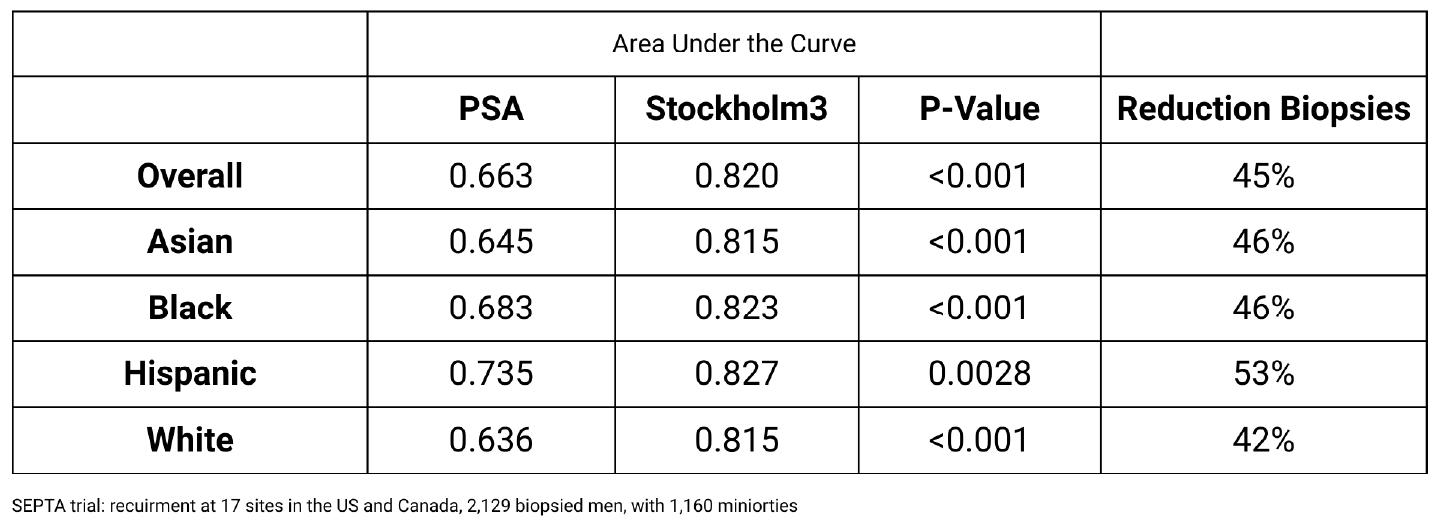
Validated across diverse populations
Stockholm3 has been prospectively validated in multiethnic cohorts in the U.S. and Canada, representing the largest evaluation of a prostate cancer biomarker in minority populations.
The test demonstrates equivalent diagnostic accuracy across all racial and ethnic groups, ensuring consistent risk discrimination for broad population screening. [12]
Contact
Stockholm3 is currently available in the following markets: The UK, Switzerland, Germany and the Nordic countries. For information on how to order the test, please contact:
Europe
Germany: Labor Dr. Wisplinghoff, e-mail: labor@wisplinghoff.de; telephone: +49 (0) 221 940 5050
Switzerland: labor team, e-mail: info@team-w.ch; telephone: +41 71 844 45 45
UK: The Doctors Laboratory, e-mail: stockholm3@tdlpathology.comTelephone +44(0) 207 307 7373
Nordics (Sweden, Norway, Finland): A3P Lab Customer Service, Uppsala, Sweden. E-mail: customersupport@a3p.com, telephone: +46 (0) 10-182 33 01
All other markets
A3P Lab customer service, Uppsala, Sweden.
E-mail: customersupport@a3p.com, telephone: +46 (0) 10-182 33 01Andreas Hoel - VP Marketing and Sales.
E-mail: andreas.hoel@a3p.com, telephone: +45 2597 4250
-
1. Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level ≤4.0 ng per milliliter. N Engl J Med. 2004;350(22):2239-2246. doi:10.1056/NEJMoa031918
2. Moller F, Mansson M, Wallstrom J, Hellstrom M, Hugosson J, Arnsrud Godtman R. Prostate Cancers in the Prostate-specific Antigen Interval of 1.8-3 ng/ml: Results from the Goteborg-2 Prostate Cancer Screening Trial. Eur Urol. 2024. doi:10.1016/j.eururo.2024.01.017
3. Eldred-Evans D, Tam H, Sokhi H, et al. An Evaluation of Screening Pathways Using a Combination of Magnetic Resonance Imaging and Prostate-specific Antigen: Results from the IP1-PROSTAGRAM Study. Eur Urol Oncol. 2023;6(3):295-302. doi:10.1016/j.euo.2023.03.009
4. McHugh JK, Bancroft EK, Saunders E, et al. Assessment of a Polygenic Risk Score in Screening for Prostate Cancer. N Engl J Med. 2025;392(14):1406-1417. doi:10.1056/NEJMoa2407934
5. Loeb S, Bjurlin MA, Nicholson J, et al. Overdiagnosis and overtreatment of prostate cancer. Eur Urol. 2014;65(6):1046-1055. doi:10.1016/j.eururo.2013.12.062
6. Gronberg H, Adolfsson J, Aly M, et al. Prostate cancer screening in men aged 50-69 years (STHLM3): a prospective population-based diagnostic study. Lancet Oncol. 2015;16(16):1667-1676. doi:10.1016/S1470-2045(15)00361-7
7. Strom P, Nordstrom T, Aly M, Egevad L, Gronberg H, Eklund M. The Stockholm-3 Model for Prostate Cancer Detection: Algorithm Update, Biomarker Contribution, and Reflex Test Potential. Eur Urol. 2018;74(2):204-210. doi:10.1016/j.eururo.2017.12.028
8. Nordstrom T, Discacciati A, Bergman M, et al. Prostate cancer screening using a combination of risk-prediction, MRI, and targeted prostate biopsies (STHLM3-MRI): a prospective, population-based, randomised, open-label, non-inferiority trial. Lancet Oncol. 2021;22(9):1240-1249. doi:10.1016/S1470-2045(21)00348-X
9. Palsdottir T, Micoli C, Eklund M, et al. Stockholm3-MRI Population-Based Screening Study: Two-Year Follow-Up. Ann Intern Med. Accepted for publication, 23 June 2026.
10. Palsdottir T, Soderback H, Jaderling F, Bergman M, Vigneswaran H, Gronberg H. The Capio Prostate Cancer Center Model for Prostate Cancer Diagnostics-Real-world Evidence from 2018 to 2022. Eur Urol Open Sci. 2024;61:29-36. doi:10.1016/j.euros.2024.01.012
11. Vigneswaran HT, Palsdottir T, Micoli C, et al. Stockholm3 Versus Prostate-specific Antigen in Prostate Cancer Screening: 9-year Outcomes Demonstrating Improved Detection of Aggressive Cancers and Reduced Overdiagnosis from the STHLM3 Trial. Eur Urol. 2026;89(1):82-90. doi:10.1016/j.eururo.2025.10.001
12. Vigneswaran HT, Eklund M, Discacciati A, et al. Stockholm3 in a Multiethnic Cohort for Prostate Cancer Detection (SEPTA): A Prospective Multicentered Trial. J Clin Oncol. 2024;42(32):3806-3816. doi:10.1200/JCO.24.00152
13. Elyan A, Saba K, Sigle A, et al. Prospective Multicenter Validation of the Stockholm3 Test in a Central European Cohort. Eur Urol Focus. 2024;10(4):620-626. doi:10.1016/j.euf.2023.09.016
14. Tilki D, Rejek N, Nohe F, Haese A, Graefen M, Thederan I. External Validation of Stockholm3 in a Retrospective German Clinical Cohort. Eur Urol Focus. 2025;11(1):82-87. doi:10.1016/j.euf.2024.07.009
15. Viste E, Vinje CA, Lid TG, et al. Effects of replacing PSA with Stockholm3 for diagnosis of clinically significant prostate cancer in a healthcare system - the Stavanger experience. Scand J Prim Health Care. 2020;38(3):315-322. doi:10.1080/02813432.2020.1802139
16. Micoli C, Crippa A, Nordstrom T, et al. Effect of a one-time sensitive screening intervention on prostate cancer mortality: The STHLM3 randomized trial. ASCO Genitourinary Cancers Symposium, San Francisco, 26-28 January 2026. J Clin Oncol. 2026;44(7_suppl).
17. Gronberg H, Eklund M, Picker W, et al. Prostate Cancer Diagnostics Using a Combination of the Stockholm3 Blood Test and Multiparametric Magnetic Resonance Imaging. Eur Urol. 2018;74(6):722-728. doi:10.1016/j.eururo.2018.06.022
18. Fredsoe J, Sandahl M, Vedsted P, et al. Results from the PRIMA Trial: Comparison of the STHLM3 Test and Prostate-specific Antigen in General Practice for Detection of Prostate Cancer in a Biopsy-naive Population. Eur Urol Oncol. 2023;6(5):484-492. doi:10.1016/j.euo.2023.07.006